CARE, NOT FRAUD:
DEFENDING MEDICAID’S HOME AND COMMUNITY-BASED SERVICES
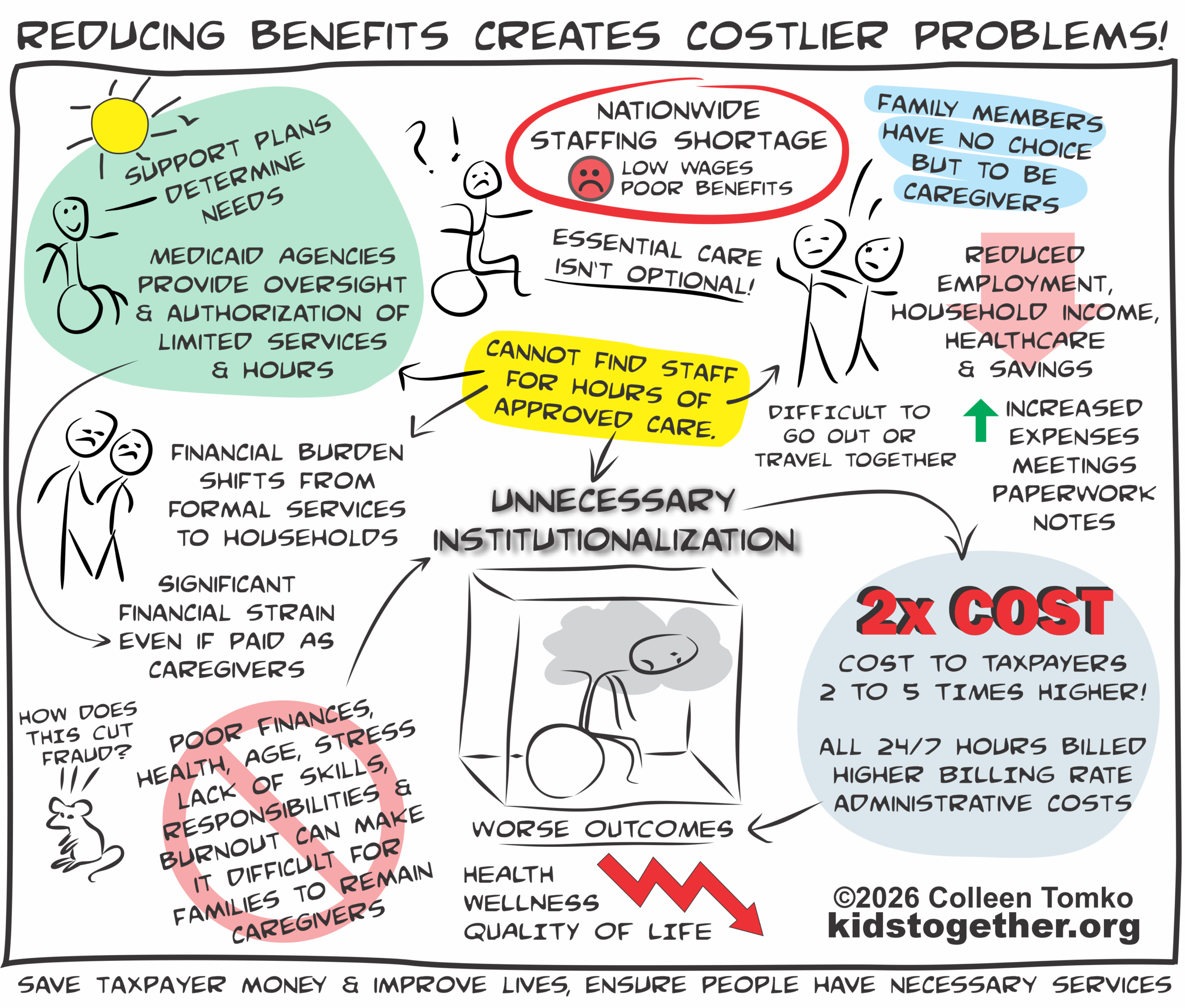
UNNECESSARY INSTITUTIONALIZATION COSTS TAXPAYERS MORE AND WORSENS OUTCOMES
People Are Forced From Their Homes and Community Due to Insufficient Funding of Community Supports
-
-
-
- The unavailability of paid staff, lack of family, or inability of family to be and/ or remain caregivers due to poor finances, health, age, stress, lack of skills, responsibilities or burnout, leaves individuals with disabilities with unmet needs and families with no choices.
-
-
History of Institutional Settings
-
-
-
- Staff complacency, high turnover, reduced health and wellness outcomes, isolation, increased costs, and fraud and waste.
- Physical, sexual, and psychological abuse are present at many residential facilities, including physical restraint and seclusion as well as the overuse and misuse of psychotropic medicine.
- Overcrowding, understaffed,
-
-
Institutions Are Not A Solution.
-
-
-
-
Institutional care costs two to five times as much as HCBS
-
-
- Full 24/7 hours billed
- Billed at much higher rates
- Administrative cost
- Overhead cost
-
-
-
-
-
-
-
-
-
Institutions lead to worse outcomes
-
-
- Decreased quality of life
- Isolation and loneliness
- Loss of autonomy and independence
- Poor health outcomes
- Greater hospitalizations
- Loss of individual legal protections as facilities gain immunity from prosecution
- Little to no transparency and accountability
-
-
-
-
-
-
-
-
-
Private equity firms are rapidly acquiring care facilities, both large and small, for profit purposes
-
-
- Equity firms cut costs to maximize profits, reducing quality
- Multi-state nature of entities makes oversight more and more challenging
- Lobby for less oversight, regulations, and immunity from legal liability for substandard care, debt, or injuries.
- Nursing and group home abuse, neglect, and deaths. “Profit, Pain, and Private Equity”
-
-
-
-
-
-
-
-
-
Institutional placements do not address fraud or reduce improper payments (not even improper payments that do end up being actual fraud), but instead make it more difficult to detect.
-
-
-
-
-
-
-
Unnecessary institutionalization violates the Americans with Disabilities Act’s ‘Integration Mandate’ by failing to provide the community-based services adults with disabilities need to remain in their communities.
-
-
-
SUPPORT PLANS DETERMINE NEEDS
Person-centered Planning Process and Functional Assessment
-
-
-
- Functional Needs Assessments are completed by trained professionals to determine needs and if the individuals meet the “Level of Care” criteria. Assessments focus on each individual, including their goals for community living.
- Individualized Support Plans are written based on assessments that specify the services, hours and supports to be provided. Plans are reviewed periodically.
- Care provided by paid staff and paid/unpaid family is considered medically necessary. It may include everything from providing personal, hygeine and health care, community integration, transportation, skill development, mobility assistance, to behavior, daily living, communication, assistive technology, and other supports.
-
-
MEDICAID AGENCIES PROVIDE OVERSIGHT AND AUTHORIZATION OF SERVICES
Strong Safeguards Already Exist to Prevent Fraud
-
-
-
- Medicaid reviews, monitors, and authorizes limited services and hours written into individual plans.
- Paid family caregivers are subject to verified strict safeguards to prevent fraud and abuse: verifications, documentation, monitoring, data analytics, background checks, evaluations, care plans, and service authorization. Additionally, Financial Management Services (FMS) companies are used as fiscal intermediaries to ensure payments to providers are in accordance with the service authorization.
- Self-direction programs allow individuals to hire staff they choose, including family. They are highly regulated to protect against waste and fraud, reduce costs, and increase positive outcomes.
- A well-administered self-direction program minimizes Medicaid fraud, waste, and abuse. Giving the fiscal and compliance responsibility to participants promotes transparency, reduces administrative overhead, and encourages sensible spending. Highly compliant, accountable, and transparent self-direction programs can deliver significant benefits to participants, their families, and budget-conscious Medicaid directors.
-
-
Research indicates that self-direction for Home and Community-Based Services (CBS) is not more prone to fraud, waste, and abuse than traditional agency-based care.
WORKFORCE REALITIES
National Staffing Shortages: Low Wages & Poor Benefits
-
-
-
- Care is essential, not optional.
- When staff are not available to hire, family members have no choice but to be caregivers, sometimes 24/7.
- Family members are forced to leave jobs, or reduce work hours, face significant losses of household income, healthcare, benefits, and savings, and increased expenses, paperwork, meetings, and notes. It is difficult for couples to go out or travel together.
- Paid family caregivers remain subject to the same requirements as any hired staff, including authorization, oversight, and paid hours limited by the approved written plan.
- When family caregivers don’t get paid for covering the approved hours, individuals are considered not utilizing the service hours and risk having their total approved hours reduced for underutilization. The decrease in approved hours is not because of reduced needs, but the inability to hire staff.
- Family caregivers provide an estimated $1 trillion in unpaid care annually (AARP Public Policy Institute), often at the expense of their own financial security and personal well-being.
-
-
Prohibiting Family Members from Being Paid Caregivers
-
-
-
- If family members are not able to get paid as caregivers to offset lost income from reductions or loss of employment, it can make it financially unfeasible to remain caregivers.
- They may be unable to provide the hours of care needed and maintain employment to pay basic bills.
- Increases the family’s need for government programs such as food assistance, housing, heating, healthcare, and other benefits, shifting expenses, not saving money.
- When individuals can’t get the care they need, it puts them at risk of forced institutionalization.
-
-
FAILURE TO ADDRESS THE NATIONAL STAFFING SHORTAGE SHIFTS THE FINANCIAL BURDEN FROM SERVICES TO HOUSEHOLDS
HOME AND COMMUNITY-BASED SERVICES (HCBS) REMAIN OPTIONAL
WITH LONG WAITING LISTS, LIMITED FUNDING & LOW STAFFING RATES
MEANWHILE, INSTITUTIONAL CARE REMAINS A GUARANTEED ENTITLEMENT
MEDICAID POLICIES CONTINUE TO HAVE AN “INSTITUTIONAL BIAS”
THE INDUSTRY OPERATES FOR A PROFIT
RESOURCES:
THIS POST WILL CONTINUE TO BE UPDATED WITH RESOURCES AND INFORMATION
SAVE THIS LINK AND RETURN FOR THE LATEST



 The
The